

ASAP 340B, the group that drug manufacturers and community health centers formed to advance a joint 340B reform agenda, recently released a two-page explainer on how their plan would change the 340B patient definition. Under it, fewer drugs prescribed at disproportionate share hospitals would qualify for 340B discounts. That’s because ASAP 340B does not consider DSH hospitals in general to be “true safety-net providers.”
The American Hospital Association, meanwhile, many of whose members are 340B DSH hospitals, recently issued a four-page backgrounder on 340B and “how it delivers value” to hospitals and “underserved patients and communities.” In its blog in April, AHA called the drug industry / health center alliance “misguided” and “self-serving.”
ASAP 340B’s new document
In early March, Pharmaceutical Research and Manufacturers of America and the National Association of Community Health Centers released 10 policy principles to guide 340B reform and launched ASAP 340B to promote them. Their 340B patient definition principle says the current definition “is overly broad and needs to be updated to protect the integrity of the program and ensure it is serving vulnerable populations.”
In early May, ASAP 340B released three targeted outreach documents on how its principles would help health centers, other 340B grantee covered entities, and rural hospitals. Each one ends with an appeal “to work with ASAP 340B to realign the 340B program in the interest of true safety-net providers and the communities they serve.”
ASAP 340B’s new patient definition document, released about two weeks ago, continues the effort. It describes six hypothetical scenarios in which drugs are dispensed. Three involve health centers, grantees, and rural hospitals. The other three involve DSH hospitals.
The three scenarios about non-hospital entities address the 340B eligibility of prescriptions written in connection with telehealth encounters and referrals to outside providers. In each scenario, the prescription would be 340B-eligible, the document says.
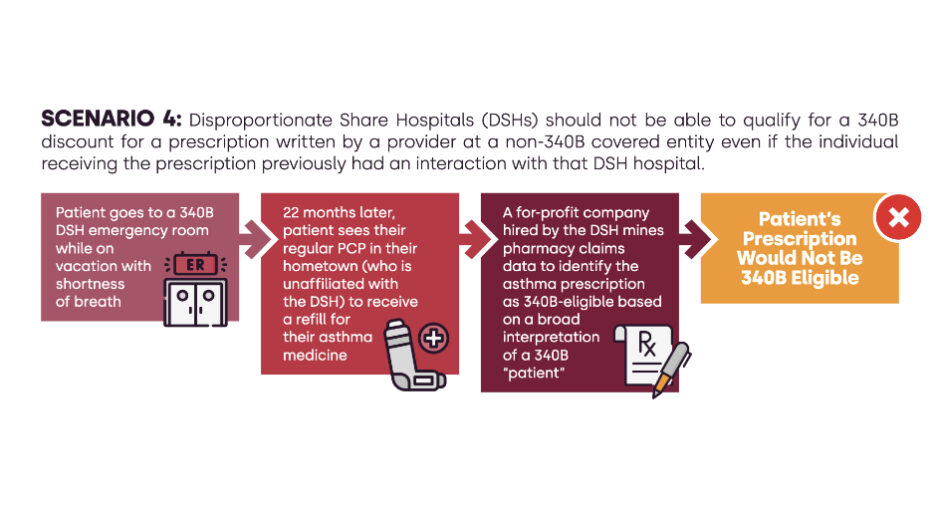
One of the three DSH hospital scenarios is about whether a hospital can qualify for a 340B discount for a prescription written by a non-340B provider because the hospital treated the same patient 22 months earlier. ASAP 340B said under its principles the prescription would be ineligible.
The second DSH scenario is about whether a prescription written at a location that is owned by a DSH but that “does not independently satisfy 340B eligibility requirements” would be 340B-eligible. ASAP 340B said it would not.
The third DSH scenario is about a prescription written at a hospital “in a medically underserved area” then filled at one of the hospital’s contract pharmacies. This time, the prescription would be 340B-eligible.
AHA’s new document
ASAP 340B’s document was intended for 340B insiders. From its content and tone, AHA’s document, released May 25, was written for those less familiar with 340B.
It opens with a history of 340B’s creation and expansion then dives into a step-by-step description of how hospitals derive revenue from 340B, starting with the manufacturer setting a drug’s price and ending with a hospital spending what it saved and earned on the drug on patient services.
The paper describes 340B’s value to hospitals next and how it ameliorates drug price inflation and public payer shortfalls. It notes that Congress did not restrict how hospitals should use their
340B savings, allowing each to decide how to best support their patients and communities. A sidebar says contract pharmacy arrangements give hospitals lacking in-house pharmacies a way to earn 340B savings. They also “provide an additional access point for patients to receive the
drugs they need, including many specialty drugs that are often in limited distribution, without patients having to travel far distances,” it says.
“The nation’s underserved patient populations rely on the 340B program to address persistent access issues for a variety of critical health care services, including access to behavioral health, telehealth and free or discounted drugs,” the conclusion says. “For every dollar in 340B sales, 340B hospitals provided over two dollars in benefit to the patients and communities they serve.”