

A message from 340B Report Publisher and CEO Ted Slafsky: We are pleased to have a sponsored content article today from Michael Gonzalez, President and Lead Consultant, FQHC340B, a valued 340B Report sponsor. I encourage you to read it. We will have more information about 340B Report sponsorship packages for 2021 very soon. In the meantime, if you have questions, feel free to reach me at ted.slafsky@340breport.com.
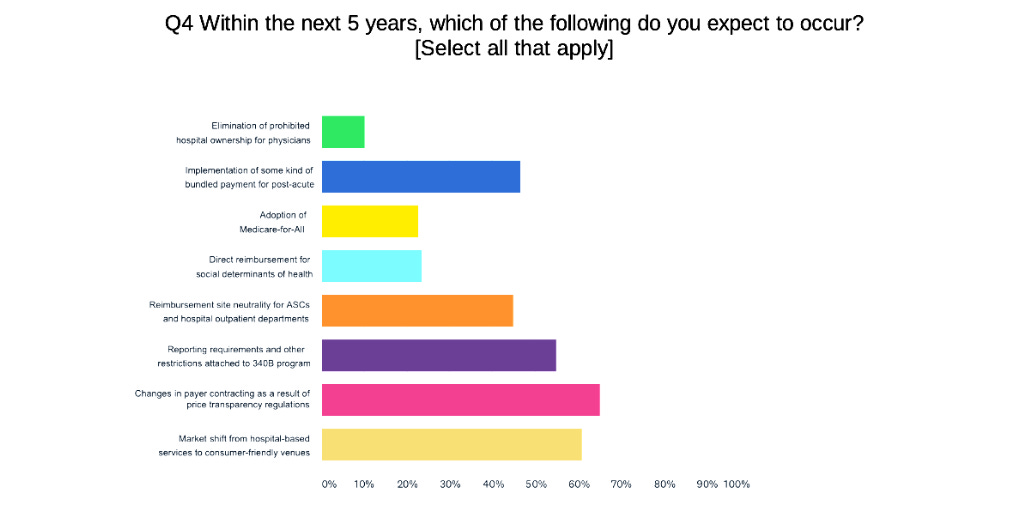
More than Half of Health Care Industry Execs Expect 340B Reporting Requirements Within Five Years
More than half (55 percent) of 130 health care industry C-suite executives surveyed expect that reporting requirements and other restrictions will be attached to the 340B program within the next five years, a health care consulting firm’s latest survey of industry executives shows. Just under half (48 percent) of the executives said an anticipated further cut in what Medicare Part B pays hospitals for 340B purchased drugs is one of the proposed regulatory changes that impacts their strategy planning most.
“The respondents are scared,” said Myron Brick, Director of Strategic Communications at Advis, the consulting firm that did the survey. “They’re frustrated that the [340B] program is misunderstood. Misinformation from program opponents is too prevalent in today’s conversations about the subject.”
“Further cuts to 340B, on top of COVID-19 financial losses, will necessitate hospitals to fundamentally rethink their delivery of care,” Brick said. “Further cuts will undoubtedly produce unforeseen consequences likely detrimental to access to care.”
Advis, which gives health systems and other providers strategic advice on 340B and other matters, asked about 340B reporting requirements and Part B cuts for 340B hospitals in its new survey, released on Oct. 6. “The stability of the 340B program is of fundamental concern to many of our clients,” Brick said. “They’ve expressed to us concern about continuing pressure on the program, some of which lacks justification. That’s why the questions were asked.” The survey was web-based and included current and former Advis clients and other company contacts.
Advis also asked the health care executives about the coming presidential election. If President Trump wins re-election, 59 percent expect to see more measures to control drug pricing. If Joe Biden defeats Trump, 42 percent expect to see more drug pricing measures. Under Trump, 75 percent expect further dismantling of the Affordable Care Act. Under Biden, 68 percent expect further strengthening of ACA. Seventy three percent also think Biden as president would support Medicare-for-All style coverage, with an opt out for commercial plans. Forty five percent see a Trump/Pence administration as better for the future of American health care, versus 41 percent who think a Biden/Harris administration would be better, with 12 percent undecided.
The Advis survey results suggests that many health care industry executives sense that the fight over 340B reporting requirements and restrictions, mostly quiet for two years, could flare up again.
In 2017-18, with the GOP controlling Congress and the White House, there was a push by the drug industry and independent oncology practices on behalf of bills to require 340B hospitals to report their 340B drug acquisition costs, revenues from all payers, payer mix information, and charity care expenses. Bills favored by the drug industry and oncology practices that compete with 340B hospitals also would have frozen disproportionate share hospital and child site enrollment in 340B for two years and toughened eligibility criteria for hospital child sites.
Democrats won control of the U.S. House in the 2018 election, the bills weren’t passed, and the push lost its momentum.
The Advis survey also suggests that health care executives anticipate further cuts in Medicare reimbursement for 340B drugs.
Oct. 5 was the deadline for public comments on a U.S. Centers for Medicare Medicaid Services’ (CMS) proposed regulation that either would keep hospitals’ Part B reimbursement for 340B drugs next year at its current average sales price (ASP) minus 22.5 percent rate (down from ASP plus 6 percent in 2017), or reduce the rate even lower, to a net ASP minus 28.7 percent rate (ASP minus 34.7 percent, plus a 6 percent add-on).
A federal appeals court this summer, in a 2-1 decision, held that CMS had authority to impose the cuts starting in 2018. Three hospital groups and three health systems with hospitals enrolled in 340B recently asked the full federal appeals court in Washington, D.C., for a rehearing. The court grants few such motions. Last year, CMS released its final rule continuing the drug reimbursement cut for 340B hospitals in 2020 on Nov. 1.
SPONSORED CONTENT
Protecting Our Patients and Safety Net in the Short and Long Term

Michael Gonzalez, President and Lead Consultant, FQHC 340B Compliance Services
So much has changed in the past few months, especially in the 340B space. Pharmaceutical manufacturers are not only putting a stress on the safety net system but are also hindering our patients lives. There are many groups advocating on behalf of the covered entities to protect 340B, but even if they are successful, we expect it will take at least a few months to get things back in order. So, the question is what should your health center do today to stay afloat?
One of the thriving services that we provide is our contract 340B coordinator service for community health centers. This service provides the health center with their own remote 340B department. This includes performing monthly audits, presenting journal entries, updating P&Ps, handling contracting, maximizing the program, preparing a monthly board report, and really handling all 340B matters. Using our expertise, we have compiled the following tips on how to navigate the current environment.
Focus extra attention on the uninsured to ensure continuity of care
We are very concerned with how the changes implemented by the manufacturers are affecting our low-income and other vulnerable patients. We have already seen this impact the lives of those patients who rely on 340B to afford their medications. I believe one of the most important things is to educate our providers on what medications are no longer available on 340B at our contract pharmacies. This gives the provider the ability to look for possible substitutions for a patient who cannot afford their medications, due to being removed from 340B pricing. If you need help with this, just reach out and I will send you a copy of the document we have utilized with our providers.
Crunch the numbers
It is more important than ever to analyze your data! If you look at e-prescription data from the EHR and 340B processed claims from your TPA, you can really understand how to maximize your program. You can also use the information to run an estimated loss analysis on claims that will no longer be processed as 340B. We have used this information to make sure we are selecting the right contracted pharmacies for those manufacturers that are requiring designations, providing management with key information needed to make decisions in these difficult times.
Look at an entity-owned pharmacy
One of my top recommendations is that management and the board of directors start discussing the possibility of opening an entity-owned pharmacy. Many health centers have relied on contract pharmacies to handle all of their 340B needs, but now we can see that it comes with the risk of losing the program. I believe that opening an entity owned pharmacy is a great hedge against the current threats. Even if contract pharmacy goes back to the way it was, it allows us to provide better care for the patient and reduce the dispensing fees for the claims captured inhouse. Many thriving health centers currently utilize both contract and entity owned pharmacies to maximize their programs.
Opening an entity owned pharmacy does come with many hurdles, including finding space to set it up, it requires a large investment, and in many cases, management does not really understand how to “manage” a pharmacy. I have partnered up with David Christian to develop a solution to combat these very common issues. Over the past few years, David and I have contracted with many centers to review the operations of their entity-owned pharmacies and provide recommendations that maximize efficiency.
We have now developed a solution to help centers pool together (saving each entity hundreds of thousands in just the initial investment) and open a remote, entity owned pharmacy. By using economies of scale, we were able to negotiate rates with vendors and provide a turnkey solution that will allow centers to own their own pharmacy. Utilizing alternative delivery sites and mail order prescriptions, this solution allows us to ensure that we take care of our patients.
For more information, please email me at mgonzalez@fqhc340b.com.
New PhRMA-Funded Paper Says 340B Contract Pharmacy Benefits For-Profit Third Parties, not Patients
A new, drug industry-funded analysis of 340B contract pharmacy over time concludes that “growth in the number of these arrangements is fueling explosive growth in the program at large and driving the 340B program farther and farther away from its original intended goal,” Pharmaceutical Research and Manufacturers of America (PhRMA) said this morning in a news release.
The paper was written by Aaron Vandervelde, Kevin Erb, and Lauren Hurley of Berkeley Research Group. Vandervelde also is the founder of Second Sight Solutions. Drug manufacturers Sanofi and Novartis are requiring, and manufacturer Merck is asking, covered entities to upload 340B contract pharmacy claims data to Second Sight’s 340B ESP platform. Sanofi on Oct. 1 stopped providing 340B pricing on drugs dispensed by contract pharmacies to covered entities that decline to provide the data.
“It is clear that contract pharmacies have leveraged market power to drive unprecedented program growth and siphon money out of the program and away from vulnerable patients,” PhRMA President Stephen J. Ubl said. “I urge lawmakers to consider the results of this analysis and pursue policies that ensure the 340B program benefits vulnerable patients rather than just line the pockets of for-profit corporations.”
Hospital group 340B Health did not respond to a request for comment on the paper.
Supreme Court Hears Case with Significant 340B Implications
The nation’s highest court heard arguments Tuesday in a case that could have a major impact on state laws barring pharmacy benefit managers (PBMs) and the payers they represent from reimbursing drugs bought through the 340B program at lower rates than other drugs.
The U.S. Supreme Court, on average, takes just under four months following arguments to decide a case. So, we might see its decision in Rutledge v. Pharmaceutical Care Management Association toward the end of February 2021.
The case involves a 2015 Arkansas law requiring PBMs to reimburse pharmacies for generic drugs at or above the pharmacies’ wholesale acquisition cost. The law also bars PBMs from paying affiliated pharmacies more than others for the same drugs. PCMA, the national trade association for the PBM industry, argued that the Arkansas law was preempted by the federal Employee Retirement Income Security Act (ERISA). Federal district and appeals courts ruled in PCMA’s favor about ERISA’s applicability. Thirty-six states have laws similar to Arkansas’ “intended to curb abusive prescription drug practices,” the state of Arkansas said in its brief filed with the Supreme Court.
Nine states have passed laws over the past two years to stop PBMs from discriminating in reimbursement, fees, or network access on the basis of a pharmacy’s participation in 340B.
Georgia was the latest to do so, in late June. The laws could be in jeopardy if the Supreme Court rules in PCMA’s favor in Rutledge. PBMs in some of these states have challenged the new 340B anti-discriminatory laws citing ERISA.
SCOTUSblog, a highly regarded independent news service about the high court, said this week’s argument before the justices “doesn’t tell us much about how the justices will decide this case, in part because of the lack of a shared conceptual framework about how to analyze the text of ERISA…. We might see a relatively splintered court, looking once again for a clear and reliable method of assessing the reach of ERISA’s preemption.”
AstraZeneca Waffles on its One Contract Pharmacy per 340B Entity Policy
Drug manufacturer AstraZeneca’s policies are in flux regarding how it is implementing its decision to stop providing 340B discounts to covered entities with their own outpatient pharmacies or to limit discounts to just one contract pharmacy for entities lacking an in-house pharmacy.
AstraZeneca announced its policy Aug. 17. Michael Gonzalez, President and Lead Consultant at FQHC 340B (a 340B Report sponsor), says he asked the company in early September how it defines “covered entity” for purposes of its one-contract-pharmacy policy. A company representative told Gonzalez in a Sept. 4 email, “Any 340B entity can designate one contract pharmacy. As long as each of your locations has a unique 340B identifier you can add one contract pharmacy for each location. For example if you have 8 locations you will be able to have up to 8 CPs to service these.”
Gonzalez has been helping clients without in-house pharmacies designate for AstraZeneca their one contract pharmacy for each location with a unique 340B ID. According to Gonzalez, AstraZeneca has been rejecting locations that do not have their own wholesaler accounts and that have not bought AstraZeneca products previously.
Health centers, he explains, typically have had bill to / ship to arrangements with their contract pharmacies, in which just one location has had a wholesaler account. AstraZeneca is now saying each location that a covered entity wishes to have a contract pharmacy must have a dedicated wholesaler account.
AstraZeneca also told Gonzalez, if a location buys from AstraZeneca “in the future, we will add the Covered Entity so they can receive 340B pricing and now have the Contract Pharmacy that will also be added as well. We don’t add anyone who can potentially purchase, only once they do purchase.”
Recent Research Digest
U.S. Insulin Prices 5x to 10x Higher in U.S. than in Other Countries
Drug manufacturers prices for insulin in the United States, not adjusted for rebates or discounts, are “often five to ten times higher” than the prices charged in other developed countries, new federally funded research by the RAND Corp. found. “The analysis suggests that U.S. insulin prices would still have been considerably higher—about four times higher—than those in other countries even when accounting for potential rebates,” RAND said.
Research published by the Health Care Cost Institute in January 2019 found that U.S. consumer spending on insulin roughly doubled between 2012 and 2016, driven by higher insulin prices (not greater utilization) and, to a lesser extent, by a shift to use of more expensive products.
Three insulin manufacturers—Sanofi, Eli Lilly and Co., and Novo Nordisk—dominate the global and U.S. markets. Two of the three—Sanofi and Lilly—are among the five drug manufacturers ending or placing restrictions on 340B pricing for drugs dispensed by contract pharmacies.
NEJM Editors Say Candidates Who Bungled COVID-19 Response Deserve Defeat at Polls
For the first time in the history of the New England Journal of Medicine, its editors are calling for the defeat of political leaders soon facing re-election, due to their mishandling this year of the COVID-19 pandemic.
“The response of our nation’s leaders has been consistently inadequate,” NEJM’s editors wrote in an Oct. 8 editorial. “This election gives us the power to render judgment…. When it comes to the response to the largest public health crisis of our time, our current political leaders have demonstrated that they are dangerously incompetent. We should not abet them and enable the deaths of thousands more Americans by allowing them to keep their jobs.”
The editorial names no specific candidates for office deserving defeat. The New York Times, The Washington Post, and USA Today, however, interpreted it as a call for President Trump’s defeat and an endorsement of Joe Biden, his Democratic rival.
Up to 7.7 Million U.S. Workers Lost Health Insurance Due to Pandemic
As many as 7.7 million workers in the U.S. lost jobs with employer sponsored health insurance as of June 2020 due to the COVID-19 pandemic, according to new research by the Commonwealth Fund, the Employee Benefit Research Institute, and W.E. Upjohn Institute for Employment Research. These workers’ insurance “covered 6.9 million of their dependents, for a total of 14.6 million affected individuals,” the study report said.
Last month, the U.S. National Center for Health Statistics released preliminary national survey data indicating that 9.7 percent of the total U.S. population lacked health insurance coverage during the first quarter of 2020, before the COVID-19 pandemic’s first wave crested.
OPPS Proposed Rule Digest
PhRMA’s Comments
Pharmaceutical Research and Manufacturers of America (PhRMA) supports the Trump administration’s proposal to reduce Medicare Part B reimbursement for drugs hospitals buy through the 340B program by another 6.2 percent starting next year, the drug industry trade association told the U.S. Centers for Medicare & Medicaid Services in comments Oct. 5 on CMS’s hospital outpatient prospective payment system (OPPS) proposed rule.
“We are concerned that much larger differentials exist between drug payments and acquisition costs for 340B hospitals compared to non-340B hospitals,” PhRMA said. “CMS’s proposal will help address the market-distorting effects of this difference and reduce cost-sharing for a significant number of Medicare patients at 340B entities.”
PhRMA also said that, while it lauds CMS’s proposal, it “is addressing only one symptom of deeper problems with the 340B program. While we recognize solutions to problems with the 340B program generally fall outside of CMS’ authority, it is vital for HHS to purse them to ensure the program fully supports true safety net providers and benefits vulnerable low-income patients. We urge HHS to consider additional steps to establish oversight and integrity in this important program and ensure it is delivering benefits to the patients and communities it is intended to serve.”
America’s Essential Hospitals Comments
In its Oct. 5 comments, America’s Essential Hospitals implored CMS to withdraw its proposal to set Part B reimbursement for hospitals’ 340B-acquired drugs at a net rate of average sales price (ASP) minus 28.7 percent.. “The payment cut is based on an unlawful application of CMS’ authority to set payment rates for specified covered outpatient drugs (SCODs) under the Social Security Act (SSA) and would have devastating consequences for vulnerable communities,” the group said. America’s Essential Hospitals is one of three hospital associations suing CMS over the cuts.
Vizient Comments
Health care group purchasing and services organization Vizient “strongly opposed” CMS’s proposal to pay “for drugs acquired under the 340B program at ASP minus 34.7 percent, plus an add-on of 6 percent of the product’s ASP.” Vizient said it was unreasonable for CMS to derive the new rate from a survey of hospitals conducted during an early, intense phase of the COVID-19 pandemic. It also said it has “significant concerns” about the survey data’s reliability.
“While Vizient supports efforts to address rising drug costs, dramatically reducing crucial Medicare payments to safety-net hospitals and health systems does not achieve that goal,” the GPO wrote. “Instead, it has a detrimental effect of impeding hospitals’ ability to utilize 340B savings to maintain programs that provide services to vulnerable populations, including Medicare beneficiaries.”
“Vizient strongly opposes any proposal that continues to significantly reduce the benefits of the 340B Program for hospitals,” it said.