

Correspondence in April and May 2020 between the 340B prime vendor and a law firm sheds more light on the start of a policy that the federal government ended abruptly last week that let hospitals start using 340B drugs at certain offsite locations sooner than it previously would allow.
Hospitals are still reeling over the U.S. Health Resources and Services Administration decision last week to end a 340B patient eligibility policy it announced three years ago as a COVID-19 flexibility but quickly said applied regardless of the pandemic. The policy said that for hospitals unable to register outpatient facilities in 340B because they are not yet on the hospital’s most recently filed Medicare cost report, “the patients of the new site may still be 340B eligible to the extent that they are patients of the covered entity.”
HRSA told 340B Report on May 5 the policy would end when the COVID-19 public health emergency ended May 11. Almost three years earlier, HRSA told 340B Report the policy was in place regardless of COVID-19. Health systems say HRSA’s policy withdrawal was wholly unexpected and undermines the financial viability of clinics they already opened or plan to open. They say the clinics can’t exist without revenue from prescribing or administering 340B drugs onsite.
Now there is documentation that the 340B prime vendor, speaking with HRSA’s authority, said in May 2020 that patients of these unregistered hospital child sites may be 340B-eligible to the extent they are patients of the parent hospital, regardless of COVID-19.
William von Oehsen, principal of Powers law firm, sent HRSA Administrator Carole Johnson a May 12 letter expressing confusion “over HRSA’s apparent withdrawal of this policy on the grounds that it only applied during the PHE.”
His letter includes an exchange of emails, dated April 20 through May 18, 2020, that he had with Katheryne Richardson, then vice president of 340B compliance at Apexus, the 340B prime vendor. She currently is vice president global healthcare strategy and pricing for Bristol-Myers Squibb.
In an April 20, 2020, email, von Oehsen asks Richardson if HRSA “would be willing to help register [a client] hospital’s new child site on an accelerated timeframe.”
Richardson replied on April 21, “Your question is similar to others that we’ve seen, and HRSA has responded consistently to it” that “until such time the site is listed on the cost report, we would note that patients of the new site may still be 340B eligible to the extent that they are patients of the covered entity. These situations should be clearly auditable and documented in policies and procedures.”
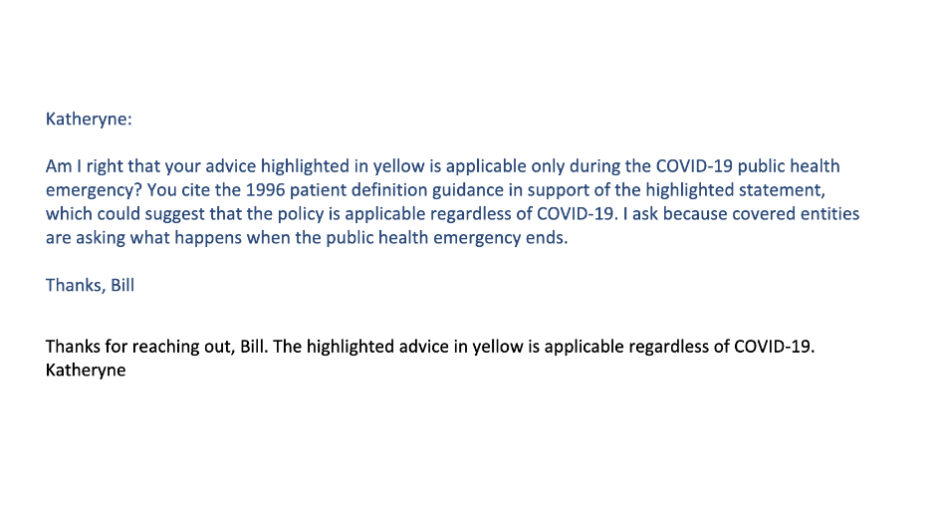
von Oehsen asked on May 18 if Richardson’s April 21 advice “is applicable only during the COVID-19 public health emergency” because she cited HRSA’s 1996 patient definition guidance, which von Oehsen said “could suggest that the policy is applicable regardless of COVID-19.”
Richardson answered the same day that the advice “is applicable regardless of COVID-19.”
Apexus reportedly has a policy of asking HRSA how to answer questions for which there is not already an approved answer, especially from legal counsel for 340B stakeholders.